B 1/7 Mahanagar Extension ( Opp. Sahara India Centre ), Kapoorthala, Lucknow - 226006
Mon - Sat: 10:00am to 8:30pm
A patient from Gomti Nagar came to Susanjeevani Hospital last month. She was 67 years old, had been diabetic for 12 years, and had noticed her central vision becoming blurry over the past few months. Her family assumed it was diabetic retinopathy. Her previous doctor had told her it might be macular degeneration. She did not know the difference — and neither did her family.
She is not alone. Every week at our eye hospital in Lucknow, we see patients — and their families — confused between these two conditions. Both affect the macula. Both damage central vision. Both can lead to permanent vision loss if not treated properly.
And yet they are fundamentally different diseases with different causes, different risk factors, different stages, and very importantly, different treatment approaches.
Getting this distinction right matters enormously — because treating one condition with the approach meant for the other is not just ineffective, it is potentially harmful. This blog gives you a complete, easy-to-understand comparison of macular degeneration and diabetic retinopathy — written specifically for patients and families in Lucknow who are trying to make sense of their diagnosis.
First — What Is the Macula and Why Does It Matter?
Before comparing the two conditions, it helps to understand the macula — because both conditions affect it.
The macula is a small but extraordinarily important area at the very centre of the retina — the light-sensitive layer at the back of your eye. It is approximately 5 millimetres in diameter and is responsible for all your sharp, detailed central vision — the vision you use for reading, recognising faces, watching television, driving, threading a needle, and seeing fine detail.
When the macula is damaged — for any reason — central vision deteriorates. You may notice a blurred or dark spot in the centre of your vision, distortion of straight lines, difficulty reading or recognising faces, or colours appearing washed out.
Peripheral (side) vision is typically preserved because the peripheral retina handles that — but central vision, once significantly damaged, is very difficult to recover.
Both macular degeneration and diabetic retinopathy damage the macula — but through entirely different mechanisms. Understanding those mechanisms is the key to understanding why these are different conditions entirely.
What Is Diabetic Retinopathy? — A Disease of Blood Sugar and Blood Vessels
Diabetic retinopathy is a complication of diabetes — type 1 or type 2. It is caused by chronically high blood sugar damaging the tiny blood vessels (capillaries) that supply the retina with oxygen and nutrients. Over years of uncontrolled or poorly controlled diabetes, these vessels weaken, leak, swell, and eventually close off — starving the retina of blood supply and triggering dangerous new vessel growth.
Diabetic retinopathy is one of the leading causes of vision loss and blindness in working-age adults in India. In Lucknow and across Uttar Pradesh — where diabetes prevalence is high and regular eye screening remains inconsistent — a significant number of patients reach our eye hospital in Lucknow with advanced diabetic retinopathy that could have been detected and treated much earlier.
Who Gets Diabetic Retinopathy?
Diabetic retinopathy can affect anyone with diabetes — type 1 or type 2. The risk increases significantly with:
- Duration of diabetes — the longer you have had diabetes, the higher the risk. After 20 years of diabetes, almost all type 1 and over 60 percent of type 2 diabetic patients have some degree of retinopathy.
- Poor blood sugar control — consistently high HbA1c levels accelerate retinal vessel damage dramatically.
- High blood pressure — hypertension compounds the damage to retinal vessels and significantly worsens diabetic retinopathy.
- High cholesterol — elevated lipids are associated with harder, more persistent retinal deposits called exudates.
- Kidney disease — diabetic nephropathy and diabetic retinopathy often progress together, as both are caused by the same underlying vascular damage.
- Pregnancy — gestational diabetes and pre-existing diabetes in pregnant women can cause rapid progression of retinopathy.
In Lucknow, we see a very high number of diabetic patients from all parts of the city — Indira Nagar, Alambagh, Mahanagar, Rajajipuram, Charbagh, Aliganj, and across the Faizabad Road and Kanpur Road corridors — many of whom have had diabetes for years without ever having had a retinal examination. This is one of the most dangerous gaps in diabetic care.
Read more on diabetic retinopathy.
Stages of Diabetic Retinopathy
Diabetic retinopathy progresses through clearly defined stages:
- Non-Proliferative Diabetic Retinopathy (NPDR) — Mild, Moderate, Severe: In early stages, small bulges called microaneurysms appear in retinal vessel walls. These leak blood and fluid into the retina, causing haemorrhages and retinal swelling. Vision may be normal or mildly affected. As NPDR advances, more vessels close off and the retina becomes increasingly ischaemic — deprived of oxygen.
- Diabetic Macular Oedema (DMO): At any stage of retinopathy, fluid can leak into the macula and cause it to swell — this is called diabetic macular oedema. It is the most common cause of vision loss in diabetic patients and can occur even in mild NPDR. It causes blurring of central vision that progressively worsens.
- Proliferative Diabetic Retinopathy (PDR): When large areas of retina become ischaemic, the body releases VEGF — triggering the growth of fragile new blood vessels across the retinal surface and into the vitreous gel. These bleed easily, causing vitreous haemorrhage — sudden, severe vision loss where patients describe their vision going dark or red. They also form scar tissue that can pull on the retina causing tractional retinal detachment — a surgical emergency.
Read more about how diabetes affects your eyes and diabetic eye disease to understand each stage in detail.
Symptoms of Diabetic Retinopathy
This is critically important — early diabetic retinopathy causes no symptoms at all. Patients feel nothing, see nothing unusual, and assume their eyes are fine. By the time vision blurs or deteriorates, significant damage has usually already occurred.
Symptoms when they do appear include blurring of central vision, floaters (dark spots or strings in vision), sudden severe vision loss (from vitreous haemorrhage), and distortion of vision.
What Is Macular Degeneration? — A Disease of Ageing and Retinal Cell Breakdown
Age-related macular degeneration — commonly called AMD or macular degeneration — is a completely different disease. It is not caused by diabetes or blood sugar. It is a progressive degeneration of the macula that occurs as part of the ageing process, caused by the breakdown and dysfunction of the specialised cells that make up the macula — particularly the retinal pigment epithelium (RPE), a layer of cells that supports and nourishes the photoreceptors.
AMD is the leading cause of severe vision loss in people above 60 years of age in developed countries, and its prevalence in India — including Lucknow — is rising as the population ages. Families in Mahanagar, Gomti Nagar, Indira Nagar, Sector C, and other established residential areas of Lucknow frequently bring elderly parents or grandparents to our eye hospital in Lucknow with complaints of blurring central vision that has developed gradually over months — and AMD is one of the most common diagnoses we make in this age group.
Who Gets Macular Degeneration?
Unlike diabetic retinopathy, macular degeneration is not caused by a systemic disease. Its main risk factors are:
- Age — the single most important risk factor. AMD is uncommon below 55 and becomes increasingly common above 65 and 75.
- Family history — AMD has a significant genetic component. If a parent or sibling has AMD, the risk is substantially higher.
- Smoking — cigarette smoking is the strongest modifiable risk factor for AMD. Smokers have 2 to 4 times the risk of developing AMD compared to non-smokers.
- Prolonged UV exposure — years of unprotected exposure to sunlight contributes to AMD risk.
- Diet poor in antioxidants — a diet low in leafy green vegetables, fruits, and omega-3 fatty acids increases AMD risk.
- Cardiovascular disease and high blood pressure — these increase AMD risk independently of diabetes.
- Light iris colour — people with blue or light-coloured eyes have slightly higher AMD risk, though this is less relevant in the Indian context where most patients have dark irises.
Types of Macular Degeneration — Dry and Wet
AMD comes in two fundamentally different forms — and understanding the difference between them is important for patients:
- Dry AMD (Atrophic AMD): This is the more common form, accounting for approximately 80 to 85 percent of all AMD cases. It involves the gradual thinning and degeneration of the retinal pigment epithelium and photoreceptors in the macula. Characteristic yellowish deposits called drusen accumulate under the macula. Vision loss is typically slow and gradual — often developing over years. There is currently no curative treatment for dry AMD, but nutritional supplements (AREDS2 formula) can slow progression in intermediate and advanced cases. Dry AMD can progress to wet AMD in some patients.
- Wet AMD (Neovascular AMD): This is the less common but more aggressive and vision-threatening form. It is caused by the growth of abnormal new blood vessels beneath the macula — a process called choroidal neovascularisation — driven by excess VEGF. These vessels bleed and leak fluid under and within the macula, causing rapid and severe central vision loss that can progress within days to weeks if untreated. This is where the connection to anti-VEGF treatment becomes critical — wet AMD is treated with anti-VEGF injections, which are also used in diabetic retinopathy but for entirely different reasons.
Symptoms of Macular Degeneration
In dry AMD, vision loss is gradual. Patients notice blurring of central vision, difficulty reading in dim light, and colours appearing less vivid. Many patients compensate unconsciously for months before seeking help.
In wet AMD, vision deterioration is rapid — sometimes occurring within days. A classic early symptom is the distortion of straight lines — door frames, tiles, telephone wires appear wavy or bent. This is called metamorphopsia and is caused by fluid lifting the macula unevenly. A dark or blank spot in the centre of vision may also develop. Any patient experiencing sudden distortion or rapid central vision loss should visit the best eye hospital in Lucknow without delay — wet AMD is a time-sensitive condition where early treatment makes a dramatic difference to outcomes.
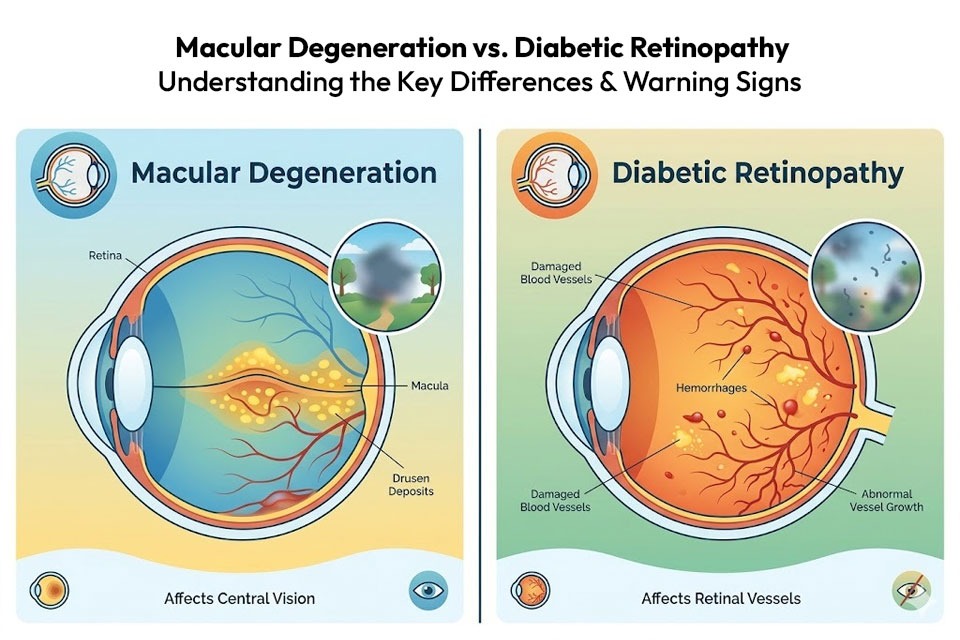
Macular Degeneration vs Diabetic Retinopathy — A Side-by-Side Comparison
This is the section most patients need — a clear, direct comparison of the two conditions:
Cause
Diabetic retinopathy is caused by diabetes — specifically by chronic high blood sugar damaging the retinal blood vessels. It will not occur in someone who does not have diabetes.
Macular degeneration is caused by age-related degeneration of the macula. It is not caused by diabetes and occurs even in people with perfectly normal blood sugar. It is driven by ageing, genetics, lifestyle factors, and oxidative damage over decades.
Who It Affects
Diabetic retinopathy affects diabetic patients — of any age, including young adults with type 1 diabetes. In Lucknow, we see diabetic retinopathy even in patients in their 30s and 40s who have had poorly controlled diabetes for many years.
Macular degeneration primarily affects people above 55 to 60 years of age. It is rare in younger patients except in cases of genetic or juvenile macular dystrophies. In Lucknow, most patients we see with AMD are above 60 — typically coming from Mahanagar, Gomti Nagar, Hazratganj, and Indira Nagar, often brought by their adult children after noticing their parent struggling with reading or watching television.
Which Part of the Eye Is Affected
In diabetic retinopathy, the entire retinal vascular network is affected — not just the macula. Haemorrhages, exudates, microaneurysms, and new vessel growth can occur throughout the retina. The macula is affected when fluid leaks into it (diabetic macular oedema) or when the disease is advanced.
In macular degeneration, the disease is confined specifically and exclusively to the macula. The peripheral retina is not affected, which is why patients with AMD retain their peripheral vision even in advanced disease — they can walk around without bumping into things, but cannot read a book or recognise a face.
Pattern of Vision Loss
In diabetic retinopathy, vision loss can be sudden (from vitreous haemorrhage in PDR) or gradual (from macular oedema in earlier stages). It typically affects the central and sometimes the overall quality of vision.
In dry AMD, vision loss is slow and gradual — progressing over months to years. In wet AMD, central vision can deteriorate rapidly over days to weeks, with characteristic distortion of straight lines as an early warning sign.
Diagnosis
Both conditions are diagnosed by a detailed examination of the retina after pupil dilation. However, the investigations used to characterise them in detail overlap significantly:
- An OCT scan is essential in both — it shows the amount and location of fluid in the macula, the thickness of retinal layers, and the presence of drusen (in AMD) or retinal swelling (in diabetic retinopathy).
- A Fundus Fluorescein Angiography maps the retinal blood vessels — showing leaking vessels in diabetic retinopathy or abnormal choroidal new vessels in wet AMD. The full FFA investigation is available in-house at Susanjeevani Hospital — one of the key reasons patients from across Lucknow and from Barabanki, Unnao, Sitapur, Hardoi, and Rae Bareli come to us for retinal diagnosis.
Treatment
This is where the two conditions differ most significantly in their management approach:
- Diabetic Retinopathy Treatment in Lucknow: The cornerstone of diabetic retinopathy management is blood sugar control — without this, no eye treatment can provide lasting benefit. Eye-specific treatments include anti-VEGF injections for diabetic macular oedema and proliferative disease, laser treatment for diabetic retinopathy (pan-retinal photocoagulation) for proliferative disease, and advanced vitreoretinal surgery for vitreous haemorrhage and tractional retinal detachment.
- Macular Degeneration Treatment in Lucknow: For dry AMD, there is currently no treatment that reverses the condition — management focuses on slowing progression with AREDS2 nutritional supplements, lifestyle modification (especially smoking cessation), UV protection, and close monitoring for conversion to wet AMD.
- For wet AMD, anti-VEGF injections are the gold-standard treatment globally. They suppress the abnormal vessel growth driving the condition, reduce macular fluid, and in many patients significantly improve vision — but they need to be given regularly over months to years to maintain their benefit. Stopping injections prematurely is the most common cause of vision loss after initially successful treatment.
Can It Be Prevented?
- Diabetic retinopathy can be significantly delayed or prevented by maintaining excellent blood sugar control from the time of diabetes diagnosis, controlling blood pressure and cholesterol, having annual dilated retinal examinations, and not smoking.
- Macular degeneration cannot be fully prevented — ageing and genetics cannot be changed. However, the risk can be reduced by not smoking, eating a diet rich in leafy vegetables and antioxidants, protecting eyes from UV radiation, maintaining cardiovascular health, and having regular eye examinations from the age of 55 onwards.
Can a Patient Have Both Diabetic Retinopathy AND Macular Degeneration at the Same Time?
Yes — and this is more common than most patients realise. An elderly diabetic patient above 60 years of age can simultaneously have diabetic retinopathy caused by their diabetes and age-related macular degeneration caused by their age. When both conditions are present together, the visual impact is compounded and the management becomes more complex — requiring careful assessment to determine the relative contribution of each condition to the patient's vision loss and to prioritise treatment accordingly.
At Susanjeevani Hospital, the best eye care hospital in Lucknow, our vitreoretinal specialist has extensive experience managing patients with concurrent retinal conditions — using OCT, FFA, and detailed clinical examination to untangle the contributions of each condition and build a personalised treatment plan.
We see patients with this dual diagnosis regularly — particularly from the older, more established areas of Lucknow like Hazratganj, Chowk, Naka Hindola, Aminabad, and Mahanagar — where elderly patients with long-standing diabetes and advancing age present with complex retinal pictures that need expert, nuanced evaluation.
The One Thing Both Conditions Have in Common — Early Detection Saves Vision
Despite all their differences, macular degeneration and diabetic retinopathy share one critically important characteristic: both cause irreversible vision damage that is far more severe and far more difficult to treat when detected late.
- In diabetic retinopathy, significant retinal damage accumulates silently for years before vision is affected. By the time a diabetic patient notices their vision is blurring, they may already have moderate to severe retinopathy. Annual retinal examination — even when vision feels completely normal — is the only way to catch this early.
- In wet AMD, the window between the first appearance of abnormal vessels and severe central vision loss can be as short as weeks to months. The characteristic warning sign — distortion of straight lines — must be acted upon immediately. Delay in seeking treatment directly translates to greater permanent vision loss.
- The Amsler grid is a simple home monitoring tool — a grid of straight lines with a central dot — that AMD patients can use daily to detect early distortion. If lines appear wavy, curved, or missing, visit the best eye hospital that same day.
Why Susanjeevani Hospital Is Lucknow's Trusted Eye Hospital for Macular and Retinal Conditions
Susanjeevani Hospital, located in Kapoorthala, Lucknow, is one of the most comprehensively equipped eye care centers in Lucknow for the diagnosis and treatment of both diabetic retinopathy and macular degeneration.
Our in-house facilities include advanced OCT imaging, Fundus Fluorescein Angiography, anti-VEGF injection therapy, laser treatment for diabetic retinopathy, and a fully equipped vitreoretinal surgical suite for advanced cases requiring surgery.
Dr. Mohit Khemchandani, our senior ophthalmologist and vitreoretinal specialist, brings deep expertise in managing the complete spectrum of retinal disease — from the earliest stages of diabetic retinopathy detected on a routine diabetic eye screening, to complex wet AMD cases requiring long-term anti-VEGF treatment protocols, to surgical cases of tractional retinal detachment and vitreous haemorrhage.
Patients come to Susanjeevani Hospital from across Lucknow — Gomti Nagar, Vibhuti Khand, Shaheed Path, Indira Nagar, Alambagh, Mahanagar, Rajajipuram, Aliganj, Charbagh — and from neighbouring districts including Barabanki, Unnao, Sitapur, Hardoi, Rae Bareli, and Lakhimpur Kheri — specifically because of the combination of advanced diagnostic equipment and experienced vitreoretinal expertise available here.
If you are a diabetic patient who has not had a retinal examination in the past year, or if you are above 55 and have noticed any change in your central vision, do not delay. Read our first-time patient consultation guide and book your appointment today.
OPD Timings: Monday to Saturday, 10:00 AM to 8:30 PM
Phone: +91-8400868388
Address: B 1/7 Mahanagar Extension, opposite Sahara India Centre, Kapoorthala, Lucknow — 226006
Easily accessible from Gomti Nagar (15 minutes), Hazratganj (20 minutes), Indira Nagar (20 minutes), Alambagh (25 minutes), Charbagh Railway Station (25 minutes), and Amausi Airport (30 minutes).